|
|
|
Prevalence
of
Hepatitis
C (HCV) Among
Military
Retirees
and
Veterans
In
Military
history
there
are
major
problems
with
the
hepatitis
B
virus
documented
in
troop
population
in
Korea
through
the
1960s.
Attack
rates
in
the
range
of 8
to
10
per
thousand
(among
50,000
troops).
This
resulted
in a
policy
of
immune
globulin
use
for
all
deployed
soldiers.
By
1970,
rates
were
one-half
to
one-third
of
the
earlier
rates.
1960s
Army
Immunization
Program
PDF
Version
In
1999
it
was
determined
by
scientists,
the
process
to
make
immune
globulin
was
inefficient
at
preventing
the
transmission
of
blood
borne
pathogens
especially
Hepatitis
C.
Hepatitis
B
immune
globulin
is
listed
as a
Red
Cross
Risk
Factor
for
transmission
of
Hepatitis
C.
Please
wait
for
the
pictures
to
load.
|
|
Of
the
26
million
retired
military
and
veterans,
almost
9
million
served
during
Vietnam
War,
more
than
3.2
million
had
active
duty
in
Asia
between
1964
and
1973.
It
is
conservatively
estimated
that
10%
(2.6
million)
are
now
infected
with
Hepatitis
C
(HCV.)
As
early
as
the
1940's,
Stokes
and
Neefe
(1945)
reported
that
epidemic
icteric
hepatitis
could
be
either
prevented
or
attenuated
by
the
parenteral
administration
of
human
serum
gamma
globulin.
In
1964,
a
program
designed
to
protect
all
military
personnel
stationed
in
Asia
against
hepatitis
was
instituted.
A
16-percent
solution
of
human
serum
gamma
globulin
in a
dose
of
0.05
ml/lb
was
used.
The
gamma
globulin
was
prepared
from
blood
donated
in
the
United
States.
A
significant
decrease
in
the
prevalence
of
hepatitis
during
that
year
as
compared
to
the
previous
year
was
seen
in
preliminary
observations
in
both
Korea
and
Vietnam.
..the
incidence
of
icteric
hepatitis
in
American
troops
hospitalized
in
Southeast
Asia
was
significantly
affected
by
the
administration
of
gamma
globulin
from
the
United
States
(Conrad
1972).
|
1942
- Yellow Fever Vaccine-Associated Hepatitis Epidemic During World War II: Follow-up More Than 40 Years Later-... it appears that about 330,000 men who received these vaccines developed HBV infection, the ratio of icteric:anicteric hepatitis being 1:7. This epidemic thus is the largest point-source hepatitis B outbreak ever recorded
- Sawyer WA Meyer KF Eaton MD Bauer JH Putnam P Schwentker FF : Jaundice in Army personnel in the western region of the United States and its relation to vaccination against yellow fever Am J Hyg 1944 ; 39 : 337-430
- Idem Jaundice in Army personnel in the western region of the United States and its relation to vaccination against yellow fever Am J Hyg 1944 ; 40 : 35-107
- Walker DW : Some epidemiological aspects of infectious hepatitis in the U.S. Army Am J Trop Med 1945 ; 25 : 75-82
- Norman JE, Mortality follow up of the 1942 epidemic of hepatitis B in the U.S. Army, Hepatology 18:790, 1993
|
|
The
Blood,
Plasma,
and
Related
Programs
in
the
Korean
War
A
plasma
program
was
also
developed
which
later
had
to
be
discontinued
because
of
the
risk
of
serum
hepatitis
associated
with
plasma
infusions
(p.
776).
The
production
of
human
serum
albumin
was
substituted
for
the
production
of
plasma
and
was
supplemented
by
the
production
of
plasma
expanders
(the
so-called
blood
substitutes
of
World
War
II).
|
|
1965
With
the
increasing
involvement
in
Vietnam
after
1965,
national
stockpiles
of
gamma
globulin
were
significantly
depleted
and
a
reassessment
of
the
prophylactic
program
was
necessary.
The
dose
of
gamma
globulin
administered
to
soldiers
was
reduced
to 5
ml
of a
16-percent
solution
after
arrival
overseas,
with
a
second
injection
5
months
later
(DA
Circ).
It
was
decided,
in
1966,
that
only
persons
under
high
risk
of
exposure
to
infectious
hepatitis
would
receive
the
inoculations
of
gamma
globulin.
A
continuing
incidence
greater
than
five
cases
per
1,000
per
year
in
particular
units
was
suggested
as a
guideline
for
this
high
risk
group.
...
the
case
rates
for
viral
hepatitis
ranged
between
4
and
10
per
1,000
troops
per
annum
(HOA).
|
1966
As
the
number
of
troops,
and
consequently
the
number
of
cases
of
hepatitis,
increased
and
the
necessity
for
air
evacuation
of
these
patients
from
Vietnam
became
apparent,
the
prolonged
period
of
treatment
and
hospitalization
not
only
caused
a
loss
of
duty
time
but
also
produced
a
logistical
problem
of
evacuation
and
replacement.
The
opening
of
the
6th
Convalescent
Center
at
Cam
Ranh
Bay,
Vietnam,
on
16
May
1966,
provided
a
way
station
to
which
hepatitis
patients
could
be
evacuated
for
convalescence.
However,
the
prolonged
recovery
phase
was
still
a
major
factor
contributing
to
the
number
of
man-days
lost
to
combat
units.
In
examining
the
problem
of
treating
hundreds
of
patients
with
infectious
hepatitis
at
the
6th
Convalescent
Center,
Repsher
and
Freebern
(1969)
were
impressed
by
the
benignity
of
the
clinical
course
in
most
of
the
patients,
the
occurrence
of
relapses
despite
adherence
to a
bed
rest
regimen... |
1969 New York Times Washington, July 28 -- The 59-year old doctor, whose companies have been blamed for the repeated use of dangerous methods and inadequate equipment, is estimated to have produced the plasma for about a fourth of an important byproduct that is widely used to protect people exposed to infectious diseases.... An executive of Cutter Laboratories once acknowledged, for instance, that gross contamination was apparent in the areas where the largest blood plasma operations were conducted. The rooms were "sloppy," he observed...When a Government doctor asked why Cutter continued to reward such an enterprise with hundreds of thousands of dollars' worth of business, the executive explained that the Stough group enjoyed crucial "contacts" with well placed officials. ......
With neither Government nor industry intruding, with most of their records held in secret, with officials passing the problem on to someone else, Dr. Stough prospered at his work throughout the nineteen-sixties. .......
|
| |
|
1969~1974 - VA - Anicteric hepatitis [HCV] has developed four times [400%]more frequently than icteric [HBV] hepatitis, the total incidence for all 6 years being 11.3%. There is indirect evidence to suggest that an undefined agent is responsible for the majority of instances of post-transfusion hepatitis occurring presently. PMID: 1235478
|
|
1972
A
large
body
of
data
is
available
from
the
Korean
era
(Conrad
1969).
Conrad
(1972)
did
a
study
of
all
soldiers
arriving
in
Korea
through
a
single
airport.
Between
May
1967
and
August
1969,
107,803
troops
were
given,
upon
arrival,
either
a
10-ml
injection
containing
2
ml,
5
ml,
or
10
ml
of a
16-percent
human
serum
gamma
globulin
or a
10-ml
albumin-sucrose-potassium
glutamate
solution.
A
second
injection
of
the
same
material
was
given
to
65
percent
of
these
soldiers
5 to
7
months
later.
Soldiers
having
symptoms
or
physical
findings
of
hepatitis
were
hospitalized
and
examined.
A
liver
biopsy
specimen
was
obtained
from
82
percent
of
the
patients.
Results
showed
467
documented
cases
of
icteric
viral
hepatitis
in
the
subjects
studied.
The
calculated
incidence
was
5.67
cases
per
1,000
among
the
control
subjects,
who
received
the
albumin,
while
among
soldiers
given
various
amounts
of
gamma
globulin
it
was
4.04
(2
ml
group),
3.39
(10
ml
group),
and
2.90
(5
ml
group)
cases
per
1,000. |
|
1977
72(1):111-21
Jan
Veterans
Administration
cooperative
study
A
randomized,
double
blind
controlled
trial
of
the
efficacy
of
immune
serum
globulin
for
the
prevention
of
post-transfusion
hepatitis.
A
Seeff
LB,
Gastroenterology
...controlled
trial
has
been
conducted
in
11
Veterans
Administration
hospitals
during
a
49-month
period
The
data
suggest,
however,
that
a
similar
reduction
in
type
non-A,
non-B
hepatitis
would
have
occurred
had
commercial
blood
been
excluded
from
use.
Furthermore,
the
efficacy
of
the
ISG,
manufactured
in
1944,
against
apparent
type
non-A,
non-B
hepatitis
suggests
that
this
overlooked
disease
has
existed
from
at
least
that
time.
Publication
Types:
Clinical
trial
Randomized
controlled
trial
More
info |
1982
J
Infect
Dis
Sporadic
non-A,
non-B
hepatitis:
frequency
and
epidemiology
in
an
urban
U.S.
population.
Alter
MJ,
et
al.
Baltimore,
Maryland
between
February
1979-August
1980.
Of
the
295
patients
with
serologically
diagnosed
hepatitis,
42%
had
non-A,
non-B
hepatitis;
|
1983
In
1983
members
of
NEPMU6
conducted
a
large
shipboard
hepatitis
study.
The
results
documented
that
sailors
and
Marines
did
acquire
hepatitis,
particularly
hepatitis
B
during
WESTPAC
deployments
(Sailors
4.9%,
Marines
6.8%).
The
data
helped
provide
scientific
justification
of
our
immunization
programs
as
carried
out
today
with
the
newer
hepatitis
vaccines.
- Navy Environmental and Preventive Medicine Unit 6 (NEPMU6) Turns Fifty
By Captain H. James Beecham III, MC, USN
- Devereux J, Haeberli P, Smithies O. A comprehensive set of sequence analysis programs for the vax. Nucleic Acids Res 1983;12:387–95.
|
|
1986
THE
ARMED
FORCES
EPIDEMIOLOGICAL
BOARD
Its
First
Fifty
Years
by
Theodore
E.
Woodward,
M.D.
...During
these
discussions,
the
Board
leaned
heavily
on
Dr.
Saul
Krugman
for
advice
and
guidance.
His
broad
and
authoritative
experience
in
the
fields
of
hepatitis
and
its
control
by
hepatitis
vaccines
has
made
him
an
important
resource,
not
only
for
the
Board,
but
also
for
the
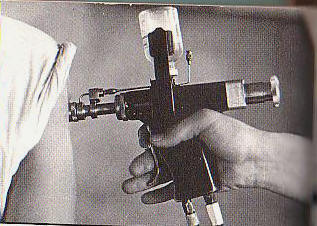
nation....During
a
Board
meeting
in
June
1986,
Captain
Michael
Stek,
Jr.,
MC,
USN,
presented
data
and
press
clippings
that
suggested
that
a
contaminated
jet
injector
gun,
which
had
been
used
at a
private
clinic
in
California
in
1985,
was
responsible
for
causing
hepatitis
in
sixty-four
patients.
The
possibility
was
also
raised
that
HIV
infection
might
be
transmitted
by
the
jet
gun
when
biological
products,
such
as
gamma
globulin,
were
administered.
After
numerous
meetings,
the
Board
recommended,
in
March
1988,
- that the jet injector gun be used only with authorized
- military technical parts and that it be sterilized
- according to standard procedures.
Veterans
Administration
cooperative
study
on
hepatitis
and
dentistry.
Am
Dent
Assoc
Sep;113(3):390-6
Schiff
ER,
Oral
and
maxillofacial
surgeons
composed
the
highest
prevalence
occupation
(24.0%),
|
|
1987
VA
also
funded
the
CDC
Vietnam
Experience
Study
published
in
1987
and
1988
Vietnam
Experience
Study
(VES)
(excerpts
from
report)
February
13,
1987
/
36(5);61-4
Current
Trends
Postservice
Mortality
Among
Vietnam
Veterans
The
CDC
has
recently
completed
the
first
phase
of
the
Vietnam
Experience
Study
(VES),
a
comprehensive
study
of
the
health
of
Vietnam
veterans.
The
VES
is a
historical
cohort
study
in
which
the
health
of
9,324
Vietnam
veterans
is
compared
with
that
of
8,989
non-Vietnam
veterans
who
served
in
Korea,
Germany,
or
the
United
States
during
the
Vietnam
era.
Eligibility
for
the
study
was
limited
to
male
U.S.
Army
veterans
who
first
entered
military
service
between
1965
and
1971,
who
served
a
single
term
of
enlistment,
and
who
were
discharged
alive
in
the
enlisted
pay
grades
E-1
through
E-5.
Participants
were
randomly
selected
from
computerized
lists
of
accession
numbers
taken
from
the
military
personnel
files
of
Army
veterans
who
were
discharged
during
the
relevant
time
period.
...this
group
of
veterans
has
not
yet
reached
the
age
at
which
chronic
diseases
have
an
important
impact
on
mortality...
Jun
7
1987
Possible
infectious
causes
in
651
patients
with
acute
viral
hepatitis
during
a
10-year
period
(1976-1985).
Liver
-
Six
hundred
and
fifty-one
patients
with
acute
viral
hepatitis
were
identified
serologically
between
January
1976
and
December
1985.
Of
these,
109
(17%)
had
hepatitis
A,
135
(21%)
had
hepatitis
B,
and
407
(62%)
had
hepatitis
non-A,
non-B.
click
here
|
|
1988
Health
status
of
Vietnam
veterans.
II.
Physical
health.
The
Centers
for
Disease
Control
Vietnam
Experience
Study.
JAMA
1988;259(18):2708-2714.
A
study
from
the
Centers
for
Disease
Control
and
Prevention
on
the
health
status
of
Vietnam
veterans
found
3%
had
used
“hard
drugs,”
including
amphetamines,
barbiturates,
cocaine,
heroin,
psychedelics,
phencyclidine
and
methaqualone.
(See
FY
1987)
Out
of
all
Vietnam
Vets
that
used
drugs
(3%
or
270,000),
90
to
95
percent
of
all
GI
users
sniffed
("snorted")
the
drug
or
inserted
a
little
in a
cigarette
and
smoked
it.
Only
13,500
are
assumed
to
have
injected
illicit
drugs
-
The Consumers Union Report on Licit and Illicit Drugs by Edward M. Brecher and the Editors of Consumer Reports Magazine, 1972 some 90 to 95 percent of all GI users sniffed ("snorted") the drug or inserted a little in a cigarette and smoked it.
-
Recreational Drug Information Website relatively few were either dysfunctional or addicted users after their return to the United States (58)
-
Hepatitis C in Vietnam Era Veterans Bradford Waters, M.D. Staff Hepatologist, Memphis VA Medical Center, Associate Professor of Medicine, University of Tennessee, Memphis 90-95% of addicts smoked heroin and only 5-10% of that group injected
-
Failure of gloves and other protective devices to prevent transmission of hepatitis B virus to oral surgeons. JAMA;259(17):2558-60 Reingold AL, Kane Department of Biomedical and Environmental Health Sciences, School of Public Health, University of California, Berkeley. A survey of 434 oral surgeons was conducted to examine risk factors for hepatitis B virus (HBV) infection. Overall, 112 (26%) of the participants demonstrated serologic evidence of past or current infection with HBV. click here
-
Centers for Disease Control. 1988. Update: Universal Precautions for Prevention of Transmission of Human Immunodeficiency Virus, Hepatitis B Virus and Other Bloodborne Pathogens in Healthcare Settings. MMWR, 37:377-382, 387, 388.
|
1989
Non-A
Non-B
hepatitis
is
identified
as
Hepatitis
C
Virus
by
the
CDC
and
Chrion
Pharmaceutical
who
would
later
possess
over
100
exclusive
rights
involving
the
Hepatitis
C
virus.
- Choo QL, Kuo G, Weiner AJ, et al. Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science 1989;244:359–62.[Abstract/Free Full Text]
- Alter HJ, et al. Detection of antibody to hepatitis C virus in prospectively followed transfusion recipients with acute and chronic non-A, non-B hepatitis. N Engl J Med 1989;321:1494-500.
-
Chiron's scientists in 1987 developed a technique to clone multiple versions of the elusive hepatitis C virus, which allows researchers to easily generate billions of viruses to research. Chiron received a patent for the discovery three years later...The CDC filed a competing patent application, listing government scientist Dan Bradley as a co-discoverer. But in 1990, the government and Bradley withdrew their claims as co-inventors and renounced all rights after Chiron paid the CDC $1.9 million and Bradley $337,500.
- Hyams KC, Palinkas LA, Burr RG. Viral hepatitis in the US Navy, 1975–1984. Am J Epidemiol 1989;130:319–26.[Abstract/Free Full Text]
|
1990
- Alter MJ, et al. Risk factors for acute non-A, non-B hepatitis in the United States and association with hepatitis C virus antibody. JAMA 1990; 264:2231-5. The incidence of non-A, non-B hepatitis remained relatively stable (average, 7.1 cases per 100,000, but there were significant changes in disease transmission patterns.
- The Pentagon revealed that the Office of the Surgeon General of the Army established a "hepatitis C registry" during the early 1990s.
According to the response, the Pentagon concluded "that hepatitis C did not constitute a significant drain on either personnel or medical resources. The Department of Defense admitted that "the registry was neither complete nor a truly random sample."...The response, written by Anne Johnson-Winegar, stated that the original intent of the registry was to:
* Maintain a list
* Track the natural progression
* Attempt to assess the impact
* Establish a database of infected persons who could be followed over time.
Data was collected from May 1990 through October 1993," said Johnson-Winegar. "Data was collected from medical treatment facility blood banks and clinical laboratories, from prevention medicine services, and from the references at WRAIR. The reporting of patient data by the preventative medicine services was mandated by OTSG, but compliance varied from post to post. In the absence of patient data from preventative medical resources, only hepatitis C virus antibody tests results were known for an individual."
While the Pentagon disbanded the hepatitis C registry for military personnel in 1993, after concluding that the infection rate was only one percent, recent studies indicate that military veterans have the highest hepatitis C rate in the nation. Statistics by the American Liver Foundation show that 1.8 percent of the U.S. population is Hepatitis C positive. Twelve to 14 percent of those infected are veterans.
- Hepatitis C Epidemiology in Military and Veteran Populations: Proceedings of the Second Biennial Conference, March 7, 1990 (1991) Institute of Medicine- Yellow Fever Vaccine-Associated Hepatitis Epidemic During World War II: Follow-up More Than 40 Years Later
- Enomoto N, Takada A, Nakao T, et al. There are two major types of hepatitis C virus in Japan. Biochem Biophys Res Commun 1990;170:1021–5.[ISI][Medline]
|
|
First
Hepatitis
C
test
was
introduced
to
the
blood
banks.
It
detected
only
46%
of
the
positive
results.
In
recent
years,
all
blood
donors
have
been
extensively
screened
by
interview
and
tested
for
a
number
of
infectious
disease
markers.
Before
1985,
donor
units
were
issued
for
transfusion
only
if
they
were
seronegative
for
syphilis
and
negative
for
hepatitis
B
surface
antigen
(HBsAg).
All
donors
had
to
successfully
complete
a
donor
interview
and
were
asked
to
voluntarily
exclude
themselves
if
they
were
in
an
AIDS
risk
group.
From
1985
through
1989,
serologic
testing
for
HIV
and
human
T-lymphotropic
virus
(HTLV)
along
with
a
more
sensitive
(second-generation)
test
for
HBsAg
were
added
to
the
testing
menu.
The
donor
interview
was
expanded
to
include
direct
questioning
about
participation
in
activities
that
put
donors
at
risk
for
HIV
or
hepatitis
infection.
Donors
were
also
tested
for
alanine
aminotransferase
and
hepatitis
B
core
antibody
(anti-HBc),
which
are
surrogate
markers
for
possible
non-A,
non-B
hepatitis.
Since
1990,
the
donor
interview
has
been
expanded
a
number
of
times,
and
serologic
testing
for
HCV
has
been
implemented.
By
the
year
2000,
a
third
generation
HBsAg
test
was
used
Beginning
in
the
spring
of
1999,
the
American
Red
Cross
and
16
member
laboratories
of
the
America’s
Blood
Centers
began
testing
donor
blood
for
the
hepatitis
C
virus
with
a
new
research
testing
method
known
as
nucleic
acid
amplification
testing
(NAT).
1991
In
1991,
OSHA
issued
the
Bloodborne
Pathogens
Standard
(29
CFR
1910.1030)
to
protect
workers
from
this
risk.
In
2001,
in
response
to
the
Needlestick
Safety
and
Prevention
Act,
OSHA
revised
the
Bloodborne
Pathogens
Standard.
The
revised
standard
clarifies
the
need
for
employers
to
select
safer
needle
devices
and
to
involve
employees
in
identifying
and
choosing
these
devices.
The
updated
standard
also
requires
employers
to
maintain
a
log
of
injuries
from
contaminated
sharps.
- van Doornum GJJ, Hooykaas C, Cuypers MT, et al. Prevalence of hepatitis C virus infections among heterosexuals with multiple partners. J Med Virol 1991;35:22–7.[ISI][Medline]
- Aach RD, et al. Hepatitis C virus infection in post-transfusion hepatitis: an analysis with first- and second-generation assays. N Engl J Med 1991;325:1325-9. - test for anti-HCV antibodies in serum samples collected between 1976 and 1979 in the Transfusion-Transmitted Viruses Study (from 1247 patients who underwent transfusion and 1235 matched control subjects who did not receive transfusions). RESULTS. Of the 115 patients...the initial serum samples of 111 were anti-HCV-negative; after hepatitis developed in these 111 patients, the first-generation EIAs detected anti-HCV in 51 (46 percent), and the second-generation assay detected anti-HCV in an additional 16 (14 percent), for a total of 60 percent. Of 40 controls, 37 were anti-HCV-negative initially,
NEW
YORK
(Reuters
Health)
-
The
findings
of a
long-term
study
of
injection
drug
users...
These
results
"underscore
the
importance"
of
nucleic
acid
screening
of
blood...an
"alarming"
34
percent
became
infected
despite
risk
reduction
counseling
click
here
MMWR.
1991;40:1-8)
The
CDC
Guideline
Recommendations
for
preventing
transmission
during
exposure-prone
invasive
procedures.
is
here:
http://www.cdc.gov/mmwr/preview/mmwrhtml/00014845.htm
"The
guidelines
stated
that
infected
health
care
workers
who
adhere
to
universal
precautions
and
who
do
not
perform
invasive
procedures
pose
no
risk
for
transmitting.
|
|
1992
-
Risk of viral hepatitis among military personnel assigned to US navy ships.
Hawkins RE, et al. J Infect Dis 1992;165:716-719
US shipboard military personnel scheduled for deployment to South America/West Africa and the Mediterranean was approximately 0.4% (9/2072).[ISI][Medline]
-
Hyams KC, Struewing JP, Gray GC. Seroprevalence of hepatitis A, B, and C in a United States military recruit population. Mil Med 1992;157:579–82.[ISI][Medline]
-
Alter MJ, et al. The natural history of community-acquired hepatitis C in the United States. The Sentinel Counties Chronic Non-A, Non-B Hepatitis Study Team. N Engl J Med 1992;327:1899-905. -
Data from the Third National Health and Nutrition Survey (1988-1994) estimate that there are approximately 3.9 million non-institutionalized, civilian Americans.
The CDC numbers do not include Veterans.
-
Donahue JG, Munoz A, Ness PM, et al. The declining risk of post-transfusion hepatitis C virus infection. N Engl J Med 1992;327:369–73.[Abstract]
-
Hyams KC, Cross ER, Bianco MA, et al. Geographic risk factors for viral hepatitis and cytomegalovirus infection among United States Armed Forces blood donors. Transfusion 1992;32:644–7.[ISI][Medline]
-
Brettler DB, Mannucci PM, Gringeri A, et al. The low risk of hepatitis C virus transmission among sexual partners of hepatitis C-infected males: an international, multicenter study. Blood 1992;80:540–3.[Abstract/Free Full Text]
|
|
1993
-
Simmonds P, Holmes EC, Cha TA, et al. Classification of hepatitis C virus into six major genotypes and a series of subtypes by phylogenetic analysis of the NS-5 region. J Gen Virol 1993;74:2391–9. [Abstract/Free Full Text]
Hepatitis
Surveillance
November
19,
1993
INACTIVATION
OF
VIRUSES
IN
BLOOD
COMPONENT
NIH
GUIDE,
Volume
22,
Number
42,
IN
VITRO
INACTIVATION
OF
VIRUSES
IN
BLOOD
COMPONENTS-
Current
risks
of
being
infected
with
a
unit
of
screened
blood
are
1 in
3,000
for
HCV,
1 in
200,000
for
HBV,
and
1 in
225,000
for
HIV.
In
addition,
viruses
such
as
the
human
T-cell
lymphotropic
viruses
(HTLV)
types
I
and
II,
and
cytomegalovirus
(CMV),
also
pose
potential
risks
Viral
Hepatitis
Surveillance
Program
1993
Centers
for
Disease
Control
and
Prevention
Issued
April,
1996
...persons
with
hepatitis
C/NANB
reported
injection
drug
use
most
frequently,
accounting
for
23%
of
cases
during
1993
...Overall,
58%
of
persons
reported
no
known
source
for
their
infection.
Dental
work
reported
as
highest
incident
for
hepatitis
non
a
non
b
- Polish LB, Tong MJ, Co RL, et al. Risk factors for hepatitis C virus infection among health care personnel in a community hospital. Am J Infect Control 1993;21:196–200.[ISI][Medline]
CONCLUSION: Although the prevalence of antibody to hepatitis C virus in health care workers was not high, needlestick injuries were associated with an increased risk for acquiring hepatitis C virus infection.
- Hyams KC, Krogwold RA, Brock S, et al. Heterosexual transmission of viral hepatitis and cytomegalovirus among U.S. military personnel stationed in the western Pacific. J Sex Transm Dis 1993;20:36–40.[ISI][Medline]
|
|
1994
Frequent
patient-to-patient
transmission
of
hepatitis
C
virus
in a
haematology
ward.
http://www.ncbi.nlm.nih.gov/pubmed/7545963?dopt=Abstract
1
Dec
94-1
Aug
95
WALTER
REED
ARMY
MEDICAL
CENTER
WASHINGTON
DC
Clinical
Impact
of
Hepatitis
C
Infection
in
Military
Active
Duty
Women-
HCV-infection
(2.7%)
is
seen
in
excess
than
the
rate
observed
among
healthy
American
blood
donors
(0.5%)
.
It
is
estimated
that
5-8%
of
the
Vietnamese
population
is
infected
with
HCV.
-
Song P, Duc DD, Hien B, et al. Markers of hepatitis C and B virus infections among blood donors in Ho Chi Minh City and Hanoi, Vietman. Clin Diag Lab Immunol. 1994:1(4):413-418.
-
Pham DQ, Walse D, Montgomery J, et al. Seroepidemiology of hepatitis C and B in an urban VA medical center. (Abstract). Hepatology 1994;326A
-
Wolfe L, Tamatsukuri S, Sayada C, et al. Detection of HCV RNA in serum using a single-tube, single enzyme PCR in combination with a colorimeteric microwell assay. In: Group Francais d'Estudes Moleculaires des Hepatites, GEMHEP, ed. Hepatitis C virus: new diagnostic tools. London, United Kingdom: John Libbey, 1994:83–94.
-
Outbreak of hepatitis C associated with intravenous immunoglobulin administration—United States, October 1993–June 1994. MMWR Morb Mortal Wkly Rep 1994;43:505–9.[Medline]
|
|
1995
The
prevalence
of
anti-HCV
among
a
cohort
of
active-duty
US
marines
stationed
in
Okinawa,
Japan
was
0.2%...
Compliance
with
universal
precautions
among
health
care
workers
at
three
regional
hospitals.
American
Journal
of
Infection
Control.
1995;23:225–236.
doi:
10.1016/0196-6553(95)90067-5.
[PubMed]
National
Institute
of
Cholera
and
Enteric
Diseases,
(e-mail:kamal412496@yahoo.com)
"this
continuous
increase
in
HCV
infection
among
IDUs,
despite
the
needle
and
syringe
exchange
programme,
is a
cause
for
concern.
The
cause
of
this
striking
increase
in
HCV
infection
is
unclear."
|
1996
- Nainan OV, Cromeans TL, Margolis HS. Sequence-specific, single primer amplification and detection of PCR products for identification of hepatitis viruses. J Virol Methods 1996;61:127–34.[ISI][Medline]
- Schreiber GB, Busch MP, Kleinman SH, et al. The risk of transfusion-transmitted viral infections. N Engl J Med. 1996;334: 1685-1690. estimated the risk of transfusion-transmitted HCV as 1 in 103,000 units transfused.
As a
result
of
the
HCV
infections
occurring
from
immunoglobulin
preparations
that
had
not
undergone
viral
inactivation,
regulatory
agencies
have
mandated
that
manufacturers
include
viral
inactivation
in
the
production
of
therapeutic
immunoglobulin.
- Lee HH, Allain JP. Genomic screening for blood-borne viruses in transfusion settings. Vox Sang. 1998;74(suppl 2):119-123.
- NUCLEIC ACID AMPLIFICATION TESTING: THE NEW INFECTIOUS DISEASE TESTING METHOD FOR DONOR BLOOD Moyne Treat Kornman, MD, German Leparc, MD, and Kaaron Benson, MD From the Florida Blood Services, Tampa, Fla (MTK, GL) and the Pathology Service at H. Lee Moffitt Cancer Center & Research Institute, Tampa, Fla (KB)...
- Brown AE, Tomlinson JP, Brundage JF, et al. The U.S. Army HIV testing program: the first decade. Mil Med 1996;161:117–22.[ISI][Medline]
- Tong MJ, El-Farra NS. Clinical sequelae of hepatitis C acquired from injection drug use. West J Med 1996;164:399–404.[ISI][Medline]
Ramsey
PW,
McConnell
P,
Palmer
BH,
Glenn
LL.
Nurses'
compliance
with
universal
precautions
before
and
after
implementation
of
OSHA
regulations.
Clin
Nurse
Spec.
1996;10:234–239.
doi:
10.1097/00002800-199609000-00008.
[PubMed]
MJA
1996;
164:
533-536
Conclusions:
Reuse
of
medical
devices
labeled
"single
use
only"
is
common...
Most
devices
appear
to
be
unsuitable
for
reuse.
Complete
cessation
of
this
practice
of
reusing
single-use
medical
devices
would
stop
potential
cross-infection,
but
this
would
cost
an
estimated
$2.5
million
or
more
per
case
prevented
|
|
1997
Did
Shots
Cause
Hepatitis
C?
Officials
Downplay
Concerns
(Star
Tribune)
"Former
Surgeon
General
C.
Everett
Koop
said
more
research
is
needed
on
all
possible
transmission
routes
for
hepatitis
C -
including
immune
globulin
inoculations."
A
four-year
review
of
patients
with
hepatitis
C
antibody
in
Department
of
Veterans
Affairs
facilities.
VA
health
care
system
in
the
Pacific
Northwest
were
tested
for
anti-HCV
antibodies,
and
8,230
(21.7%)
were
positive.
21%
had
markers
of
hepatitis
C
virus
infection...
45.8%
of
the
seropositive
veterans
were
between
the
ages
of
40
and
49
years.
There
were
6,600
HCV
cases
reported
in
the
VA
system
in
1991.
By
1994,
this
number
had
increased
to
18,854.
Over
the
next
four
years,
the
annual
number
of
newly
identified
cases
increased
steadily
to
20,203
in
1995,
21,424
in
1996,
24,850
in
1997,
and
29,799
in
1998.
Since
March
1999,
over
69,000
additional
cases
have
been
identified.
VA
officials
expect
this
number
to
continue
to
increase
substantially.
- Roselle GA, Danko LH, Mendenhall CH. A four-year review of patients with hepatitis C antibody in Department of Veterans Affairs facilities. Mil Med. 1997;162(11):711-714.
- Department of Veterans Affairs. Veterans Health Administration. Washington, D.C. 1998
Kralovic S, Roselle GA, Simbartl L, et al. Hepatitis C virus antibody (HCAb) positivity in Department of Veterans Affairs (VA) facilities. Presented at the Ninth Annual Scientific Meeting of the Society for Healthcare Epidemiology of America (SHEA). San Francisco, California. 1999. A large multi-center VA study involving twenty six Medical Centers and approximately 5,800 patients was initiated by the San Francisco VA Medical Center to study demographic factors and treatment response in VA patients.
- Spolarich AW, Russo B. Hepatitis C and veterans. December 1998/January 1999. The VVA Veteran®... screening program that tested 200 apparently healthy leaders of the Vietnam Veterans of America found 9% of those tested were infected with HCV. A more recent screening at a Vietnam Veterans’ stand down found 36% of those screened tested positive for HCV.
- Army Medical Surveillance Activity. Guidelines for use of specimens stored in the DoD serum repository. June 25, 1997. (http://amsa.army.mil/AMSA/amsa_home.htm).
|
CNN- Millions unaware they have hepatitis C
The newly appointed surgeon general, David Satcher, speaks to the House subcommittee "We know that many Americans infected ...unaware that they have the disease,"
§Former surgeon general Koop
§"Many with hepatitis C virus have no reason to believe they are infected,“
§"Many of those at high risk are average people – §middle-aged housewives who had a cesarean section delivery, §young adults who had transfusions as high-risk babies or §middle-aged
men who served in Vietnam." ...
Letters will be sent to anyone who received blood from a donor who later tested positive for hepatitis C
Rep. Christopher Shays ¡Public concerns about hepatitis C have been overshadowed by AIDS.
For too long it has been ... characterized as a disease confined to intravenous drug users..." "It wasn't five years ago. Our guard wasn't up
|
Late M. A ction urged to stem hepatitis C. US Med 1998;34:3, 42, 43.
July 19, 1998
House Committee On Veterans' Affairs Subcommittee On Benefits
Statement Of LEONARD B. SEEFF, M.D.
National Institutes Of Diabetes, Digestive, And Kidney Diseases
National Institutes Of Health
And Former Chief, Gastroenterology & Hepatology
Veterans Affairs Medical Center, Washington, D.C.
The only large, population-based screening study in the VA of which I am aware is one that was conducted at my VA Medica2355l Center here in Washington, DC over a 6-week period at the beginning of 1994. The intent of our study was to screen 1,000 consecutive patients who were admitted to the facility, regardless of which section they entered, for the presence of hepatitis B and hepatitis C markers. We accomplished our aim in 839 patients and were astonished to find that, whereas 3% were infected with hepatitis B, 21% had markers of hepatitis C virus infection....Furthermore, test procedures were changing during this period and the data did not take into account the important issue, at that time, of false-positive results....persons seen in the emergency room at Johns Hopkins University, in which a prevalence figure of 18.5% was noted. The populations studied in these two screening surveys both derived from the "inner city" and both identified parenteral drug abuse as the apparently most common risk factor....Obviously, these results cannot be applied to other VA Medical Centers...
NAT- the false positive Hepatitis C test for batch blood testing- Approximately 50% of the samples found to be NAT-positive are expected to be false positive (ie, no positive individual donation can be identified).
-
NUCLEIC ACID AMPLIFICATION TESTING: THE NEW INFECTIOUS DISEASE TESTING METHOD FOR DONOR BLOOD Moyne Treat Kornman, MD, German Leparc, MD, and Kaaron Benson, MD From the Florida Blood Services, Tampa, Fla (MTK, GL) and the Pathology Service at H. Lee Moffitt Cancer Center & Research Institute, Tampa, Fla (KB)...
-
NAT Implementation. Bethesda, Md: American Association of Blood Banks; 1999. American Association of Blood Banks Association Bulletin #99-3 NAT could theoretically close the window period of HCV from the current 70 to 80 days to approximately 10 to 30 days. This would reduce the risk of transfusion-transmitted HCV from approximately 1 in 100,000 units transfused to 1 in 500,000-1,000,000 units transfused.
October 15, 1998
House Report 105 HR 820
DAN
BURTON,
Indiana,
Chairman-
Seventh
Report
By
The
Committee
On
Government
Reform
And
Oversight
51
351
CC
Union
Calendar
No.
461
105th
Congress,
2d
Session
HEPATITIS
C:
SILENT
EPIDEMIC,
MUTE
PUBLIC
HEALTH
RESPONSE
Between
1995
and
1997
the
annual
number
of
newly
identified
persons
rose
from
20,203
to
21,424
to
24,850.
In
1998
an
additional
29,799
unique
cases
were
recorded
within
the
VA.
Of
all
veterans
in
the
VA
system
testing
positive
for
hepatitis
C,
64%
were
Vietnam
Era
veterans.
The
mean
age
of
HCV
infected
veterans
is
49
years.
VA researcher Dr. Gary Roselle reports HCV infection in VA has increased 285% during the 4 year period Roselle states; “Since most veterans are not treated in VA medical facilities, the actual incidence of HCV infected veterans is undoubtedly much greater.”
- Former Surgeon General C. Everett Koop – ¡HCV screening program for all U.S. military personnel… ¡all possible transmission routes for hepatitis C - including ¡more research is needed on immune globulin inoculations...begin screening troops for hepatitis C.
"You've got a demon on your hands," he said. "You'd better find out where that's coming from if you can."
|
- Senator Richard Shelby (R AL) asked the Pentagon to look further into the possibility that immune globulins may have spread HCV. The Pentagon did not agree to study the issue and Senator Shelby inserted the following report language in the 1998 Department of Defense Appropriations bill: ``The Department of Defense shall determine rates of hepatitis C infection among personnel who served in deployments overseas or who received blood plasma products from individuals infected with hepatitis C and provide counseling and access to treatment for personnel as needed.''\33\
November
1998
Presentation
of
Gay
Roselle
to
the
Veterans
of
Foreign
Wars.
April
9,
1999.
Washington,
DC.
~
Spolarich
AW,
Russo
B.
“Hepatitis
C
infection
in
apparently
healthy
Vietnam
Era
veterans.”
Submitted
for
publication.
|
|
1998
-
Bray RM (project director). 1998 Department of Defense survey of health related behaviors among military personnel. Research Triangle Park, NC: Research Triangle Institute, February 1999.
-
Bachman JG, Freedman-Doan P, O'Malley PM, et al. Changing patterns of drug use among US military recruits before and after enlistment. Am J Public Health 1999;89:672–7.[Abstract/Free Full Text]
October
16,
1998
CDC
MMWR,
Recommendations
and
Reports:
/
47(RR19);1-39
Enclosure
3
Proposed
Hepatitis
C
Virus
(HCV)
Antibody
Screening
Policy
Hepatitis
C
is
transmitted
primarily
by
injections
of
contaminated
blood.
The
following
are
the
possible
sources
of
hepatitis
C
infection.
If
you
can
answer
"yes"
to
any
of
these
risk
factors
and
have
not
previously
been
tested
for
hepatitis
C,
you
should
receive
a
simple
blood
test
to
determine
if
you
could
have
hepatitis
C.
-
Receiving a transfusion of blood or blood products before 1992
-
Ever injecting illegal drugs, including use once or a few times many years ago
-
Receiving clotting factor concentrates produced before 1987
-
Having been on chronic (long-term) hemodialysis
-
Being told that you have persistently abnormal liver enzyme tests (alanine aminotransferase) or an unexplained liver disease
-
Receiving an organ transplant before July 1992
-
Having a needlestick, sharps or mucosal exposure to potentially HCV-infected blood as part of your occupational duties
Please
note
and
compare
the
current
CDC
plan.
CDC
Recommendations
for
Prevention
and
Control
2001
National
Hepatitis
C
Prevention
Strategy
"Most
risk
factors
associated
with
transmission
of
HCV
in
the
United
States
were
identified
in
case-control
studies
conducted
during
1978-1986.
Risk
factors
included:
- Blood transfusion,
- Injecting-drug use
- Employment in patient care
- Clinical laboratory work
- New Exposure to a sex partner
- New Household member
- New Multiple sex partners
- New Low socioeconomic level
It's
your
fault
your
sick:(
CDC state in both reports: "These studies reported no association with military
service
or
exposures
resulting
from
medical,
surgical,
or
dental
procedures,
tattooing,
acupuncture,
ear
piercing,
or
foreign
travel.
If
transmission
from
such
exposures
does
occur,
the
frequency
might
be
too
low
to
detect"
NOTE:
2004
Statement
Of
Lawrence
R.
Deyton,
Md,
Msph-
Chief
Consultant,
Public
Health
Strategic
Health
Care
Group-
Veterans
Health
Administration-
Department
Of
Veterans
Affairs-
VA
efforts
in
hepatitis
C
have
benefited
from
close
collaboration
and
partnership
with
Veterans
Service
Organizations
and
other
veteran
and
non-profit
groups,
as
well
as
with
other
government
agencies
such
as
the
National
Institutes
of
Health
(NIH),
the
Centers
for
Disease
Control
and
Prevention
(CDC),
and
the
Federal
Bureau
of
Prisons
(FBOP).
The
CDC
continues
to
state
there
is
no
association
with
military
service
and
Hepatitis
C.
Also
note:
Red
Cross
Risk
Factors
March
5,
1998
The
newly
appointed
surgeon
general,
David
Satcher,
speaks
to
the
House
subcommittee
"We
know
that
many
Americans
infected
...unaware
that
they
have
the
disease,"
"Many
with
hepatitis
C
virus
have
no
reason
to
believe
they
are
infected,"
Koop
said.
"Many
of
those
at
high
risk
are
average
people
--
middle-aged
housewives
who
had
a
cesarean
section
delivery,
young
adults
who
had
transfusions
as
high-risk
babies
or
middle-aged
men
who
served
in
Vietnam."
|
|
1999
On
January
27,
1999
the
VA,
“announced
major
initiatives
to
respond
to
the
Hepatitis
C
virus
(HCV)
epidemic
in a
comprehensive
and
consistent
manner
across
its
(VA’s)
nationwide
health-care
system.”
The
VA’s
5-point
strategic
initiative
to
respond
to
HCV
included:
patient
education;
health
care
provider
education;
epidemiologic
assessment;
treatment;
and
research.
The
plan
in
part
called
for
“Two
new
‘Hepatitis
C
centers
of
excellence,’
to
be
located
at
VA
medical
centers
in
Miami
and
San
Francisco
to
coordinate
treatment
and
research
efforts,
as
well
as
develop
education
for
patients
and
their
families,
health-care
providers,
and
counselors
who
will
advise
patients
prior
to
and
following
testing.”
On
March
17,
1999,
the
Department
of
Veterans
Affairs
(VA)
conducted
a
nationwide
surveillance
activity
and
tested
over
26,000
veterans
for
hepatitis
C.
The
testing
revealed
a
prevalence
rate
of
6.6
percent
with
a
wide
variation
by
geography
and
era
of
military
service.
NOTE:
A
paper
published
by
Roselle
et
al.
reported
the
findings
from
this
surveillance
activity
January
1999,
VHA
established
two
Centers
of
Excellence
in
Hepatitis
C
located
at
the
VA
Medical
Center
Miami,
FL,
and
the
VA
Medical
Center,
San
Francisco,
CA.
Pueschel
M.
VHA
hepatitis
C
costs
placed
at
$250
million.
US
Med
1999;35:2,
52.
106
Congress-
Two
House
Bills
H.
R.
1020
SNYDER
Veterans'
Hepatitis
C
Benefits
Act
of
1999
establish
a
presumption
of
service
connection
for
the
occurrence
of
hepatitis
C in
certain
veterans
.
(1)
Transfusion
of
blood
or
blood
products
before
December
31,
1992.
(2)
Blood
exposure
on
or
through
skin
or
mucous
membrane.
(3)
Hemodialysis.
(4)
Tattoo
or
body
piercing
or
acupuncture.
(5)
Unexplained
liver
disease.
(6)
Unexplained
abnormal
liver
function
tests.
(7)
Working
in a
health
care
occupation.
Referred
to
the
Committee
on
Veterans'
Affairs
HR
4751
IH
>
H.
R.
1020>
HCON
130
IH –
nH. R. 5132 FRELINGHUYSEN
Veterans Comprehensive Hepatitis C Health Care Act
establish a comprehensive program for testing and treatment of veterans for the Hepatitis C virus.
(A) each veteran who served in the active military, naval, or air service during the Vietnam era and is enrolled to receive care under section 1710 of this title who requests the test or is otherwise receiving a physical examination or any care or treatment from the Secretary; and
(B) to any other veteran who requests the test.
(2) After the end of the one-year period referred to in paragraph (1), the Secretary shall provide a blood test for the Hepatitis C virus to any veteran who presents one or more risk factors for that virus and who requests the test.
Referred to the Committee on Veterans' Affairs H. R. 5132 >H. R. 639
Alter MJ, et al. The prevalence of hepatitis C virus infection in the United States, 1988 through 1994. N Engl J Med 1999;341:556-562
1999
As
ordered
by
Congress
Click
here
to
read
complete
report
Results
of
DoD
Investigations
Office
of
the
Assistant
Secretary
of
Defense
--
Health
Affairs,
the
Pentagon;
Washington,
DC
Serological
Survey
-
Vietnam era personnel: 1000 personnel currently on active duty who had been serving in the military since January 1, 1974.
(Note: This is the end of the Vietnam era, and right after the military stopped administering the reusable small pox needle and small pox vacation by Jetgun)
-
Active duty retirees with at least 20 years of military service: 2000 individuals.
(Note: at least = 1980)
(Note:
.
Rather
than
determining
rates
of
hepatitis
C
infection
among
personnel
who
"served"
in
deployments
overseas
or
who
received
blood
plasma
products
as
ordered
by
Congress,
the
1999
Senate
Armed
Services
Committee
directed
DoD
to
study
the
extent
of
service-connected
hepatitis
C
infection...during
separation
and
retirement
physicals
of
active
duty.
The
Vietnam
Era
is
considered
to
have
begun
in
1964
and
ended,
some
say,
1973.
But
the
veterans,
that
served
during
the
Vietnam
era
from
1964
until
1973,
were
basically
excluded
from
these
results.
Nobody
tested
the
immune
globulin,
the
ingredient
used
in
many
different
vaccines.
In
1999
it
was
determined
by
scientists,
the
process
to
make
immune
globulin
was
inefficient
at
preventing
the
transmission
of
blood
borne
pathogens.)
New
research
show
method
for
making
immunoglobulins
did
not
kill
the
Hepatitis
C
virus
-
Hepatitis C Virus Infection Among U.S. Military Personnel: An Assessment Of Risks and Screening Strategies- Office of the Assistant Secretary of Defense -- Health Affairs, the Pentagon; Washington, DC
April 5, 1999
-
Hepatitis C Surveillance Day in the Veterans Health Administration of the Department of Veterans Affairs. Kralovic SM, et al. National Mil Med 2002;167:756-759. ...
-
Alter MJ, et al. The prevalence of hepatitis C virus infection in the United States, 1988 through 1994. N Engl J Med 1999;341:556-562
Data from the Third National Health and Nutrition Survey (1988-1994) estimate that there are approximately 3.9 million non-institutionalized, civilian Americans who have been infected with HCV. Of these, 2.7 million have chronic infection, making HCV the most common chronic blood-borne infection in the United States. Perhaps the majority of those infected are unaware of their infection because they do not currently have signs or symptoms of disease. The highest prevalence of infection is found among those with repeated, direct percutaneous exposures to blood...The estimated prevalence of infection varies greatly among different geographic locations and selected populations in the United States according to the varying prevalence of risk factors for infection.
-
2000
To
follow
up
on
its
initiative,
the
Veterans
Health
Administration
(VHA)
issued
directive
2000-019
on
July
19,
2000,
mandating
the
installation
and
use
of
software
on
clinical
reminders
to
support
the
Hepatitis
C
reporting
process.
(Attachment
4,
p.
1)
The
VA’s
Emerging
Pathogens
Index
(EPI)
registry
is
used
to
track
the
incidence
of
HCV
in
the
VA
system.
VA
claims
it
is
now
able
to
track
veterans
who
tested
positive
for
HCV
in
each
of
the
22
Veterans
Integrated
Service
Networks
(VISNs)
on a
quarterly
and
annual
basis.
(Attachment
2,
p.
7)
However,
VA
admits,
“the
true
prevalence
of
HCV
in
veterans
who
utilize
medical
care
services
is
unknown.”
(Attachment
2,
p.
12)
VA
attributes
this
to
“deficiencies
in
data
(due
to
both
gaps
in
our
[VA]
knowledge
about
the
epidemiology
of
hepatitis
C in
the
VA
population
as
well
as
limitation
in
available
data
collection
systems).”
(Attachment
2,
p.
11)
-
April 13, Testimony of Gary A. Roselle, M. D. - 81% of all Military attending VA clinics and positive for Hepatitis C are from the Vietnam and Post Vietnam Era.
http://hcvets.com/data/hepatitis_c_in_vietnam_era_veter.htm
-
Under Secretary for Health designated an additional $20 million to be distributed to the 22 Veterans Integrated Service Networks (VISNs) for outreach, testing, counseling, and treating veterans with hepatitis
-
Public Health Strategic Health Care Group, the National Hepatitis C Program was created
-
National Hepatitis C Technical Advisory Group was created
-
Miss America 2000 Shuts Down Times Square in Honor of the American Hero - New York Is Next Stop for Hepatitis C Awareness Campaign
NEW YORK, June 29 /PR Newswire/ -- Miss America 2000, Heather French, will be in New York City's Times Square on Monday July 3 as part of her national disease awareness campaign entitled "Helping Veterans Fight a Silent Enemy: Hepatitis C." Miss French joins NYC 2000 and the New York City Mayor's Office as co-host of the "Salute the American Hero" music tribute to urge veterans to get tested for a potentially fatal virus, hepatitis C.
-
The Global Infectious Disease Threat and Its Implications for the United States
NIE 99-17D,
...a White House-appointed interagency working group identified at least 29 previously unknown diseases that have appeared globally since 1973, many of them incurable... Alone or in combination, war and natural disasters, economic collapse, and human complacency are causing a breakdown in health care delivery and facilitating the emergence or reemergence of infectious diseases.
-
Risk factors for hepatitis C virus infection in United States ...
Comment in: Hepatology. 2000 Mar;31(3):790-1. Click here to read Risk factors
for hepatitis C virus infection in United States blood donors. ...
-
VA
received
$195
million
for
screening
and
treating
patients
with
HCV
for
FY
2000.
On
June
28,
2000,
Dr.
Thomas
Garthwaite,
the
Under
Secretary
for
Health,
granted
an
additional
$20
million
to
be
distributed
to
the
22
Veterans
Integrated
Service
Networks
(VISNs)
in
order
to “
recognize
the
geographic
differences
in
the
prevalence
of
hepatitis
C
and
to
provide
incentive
to
VA
health
care
facilities
to
aggressively
outreach,
screen,
diagnose
and
treat
hepatitis
C.”
The
letter
stated:
-
“In order to recognize the geographic differences in the prevalence of Hepatitis C and to provide incentive to VA health care facilities to aggressively outreach, screen, diagnose, and treat Hepatitis C, I have made the decision to provide $20 million from the National Reserve Fund to the Veterans Integrated Service Networks (VISNs) based on each network’s Hepatitis C costs during the first two quarters of FY 2000. It is important to note that funds allocated under the Veterans Equitable Resource Allocation (VERA) will continue to be expended by each VISN to support the costs of veterans with Hepatitis C. This $ 20 million simply supplements those funds.” Letter to Chairman Shays from Dr. Garthwaite on additional funding for selected VISNs to supplement approved budgets for the Hepatitis C testing and treatment programs (6/28/00).
In
recognition
of
the
high
cost
of
treating
HCV
infection,
VA
decided
Hepatitis
C
patients
on
drug
therapy
would
be
funded
at
the
complex
care
level,
starting
in
FY
2001.
This
new
classification
will
help
medical
centers
offset
the
costs
of
treating
Hepatitis
C
patients
on
drug
therapy.
It
was
not
until
June
2000
when
VA
released
$20
million
from
the
National
Reserve
Fund
to
the
Veterans
Integrated
Service
Networks
(VISNs)
based
on
each
network’s
Hepatitis
C
costs
during
the
first
two
quarters
of
FY
2000,
that
managers
and
providers
became
aware
of
funding
for
HCV
costs.
It
is
for
this
reason
some
believe
funding
for
HCV
expenses
should
be
earmarked
and
separate
from
the
general
medical
care
resource
distribution
process.
VA
spent
$14
million
of
the
$21
million
budgeted
for
HCV
screening
and
testing
in
FY
2000.
VA
believes
the
shortfall
may
be
attributable
to
the
use
of
“untested
assumptions”
in
budget
estimates
regarding
the
number
of
veterans
who
would
need
to
be
screened
for
Hepatitis
C.
Or,
the
number
screened
may
be
underreported
due
to
inadequate
data
systems.
(Attachment
9 p.
3)
However,
these
reasons
do
not
explain
why
VA
has
still
not
been
able
to
test
more
than
20%
of
patients
using
VA
health
facilities.
There
are
also
concerns
as
to
why
VA
did
not
make
it a
point
to
notify
networks
of
the
funds
available
to
screen
and
test
patients
for
HCV,
since
VA
was
aware
network
directors
and
providers
were
concerned
about
costs.
VA
has
acknowledged
concerns
for
HCV
costs
may
effect
the
screening
of
patients.
This
was
noted
in
VA’s
White
Paper
to
Inform
Congress
on
Decisions
for
Hepatitis
C
Funding
in
which
VA
stated,
“we
cannot
be
certain
that
local
choices
regarding
allocation
of
available
resources
amongst
a
number
of
critical
patient
care
areas
have
not
created
potential
disincentives
to
the
diagnosis
and
treatment
of
hepatitis
C
infection.”
2001
On
February
27,
2001,
the
VHA
issued
directive
2001-009
entitled
“National
Hepatitis
C
Program.”
The
purpose
of
the
directive
was
to
compile
all
VHA
policies
and
programs
on
Hepatitis
C
and
to
outline
specific
requirements
for
implementing
the
program.
The
directive
also
states
“each
VA
medical
center
Director
must
designate
a
Hepatitis
C
Lead
Clinician
to
be
the
point
of
contact
for
all
clinical
Hepatitis
C
communication
and
reporting
between
the
facility,
the
Hepatitis
C
Program
office
and
other
program
offices.”
(Attachment
5,
p.
1-3)
Prevalence
and
Incidence
of
Hepatitis
C
Virus
Infection
in
the
US
Military:
A
Seroepidemiologic
Survey
of
21,000
Troops
Kenneth
C.
Hyams1,
James
Riddle2,
Mark
Rubertone3,
David
Trump2,
Miriam
J.
Alter4,
David
F.
Cruess5,
Xiaohua
Han4,
Omana
V.
Nainam4,
Leonard
B.
Seeff6,
John
F.
Mazzuchi2
and
Sue
Bailey2
Because
of a
high
prevalence
of
hepatitis
C
virus
(HCV)
infection
(10–20%)
among
veterans
seeking
care
in
Department
of
Veterans
Affairs
(VA)
hospitals,
current
US
military
forces
were
evaluated
for
HCV
infection.
Banked
serum
samples
were
randomly
selected
from
military
personnel
serving
in
1997
and
were
tested
for
antibody
to
HCV
(anti-HCV).
Overall
prevalence
of
anti-HCV
among
10,000
active-duty
personnel
was
0.48%
(5/1,000
troops);
On
the
basis
of
the
findings
from
our
study,
which
showed
a
consistently
higher
prevalence
of
HCV
infection
in
older
service
members,
DoD
has
implemented
a
targeted
risk-based
HCV
screening
program
using
Centers
for
Disease
Control
and
Prevention
screening
guidelines
for
persons
who
are
35
years
of
age
or
older
and
are
separating
or
retiring
from
military
service
(1
-
Recommendations for prevention and control of hepatitis C virus (HCV) infection and HCV-related chronic disease. MMWR Morb Mortal Wkly Rep 1998;47:1–39.[Medline]
-
B. R. Burnham
RE: "PREVALENCE AND INCIDENCE OF HEPATITIS C VIRUS INFECTION IN THE US MILITARY: A SERO-EPIDEMIOLOGIC SURVEY OF 21,000 TROOPS"
Am. J. Epidemiol., April 15, 2002; 155(8): 778 - 779.
[Full Text] [PDF]
Screening
for
risk
factors
involves
asking
a
variety
of
questions.
Current
VHA
policy
enables
veterans
to
be
tested
for
HCV
infection
if
they
desire
to
be
tested,
or
if
they
have
one
or
more
of
the
following
risk
factors:
-
1.Vietnam-era veterans (as defined by dates of service or in the age range of 40-55 years)
2. received a blood transfusion before 1992,
3. past or present intravenous drug use,
4. unequivocal blood exposure of skin or mucous membrane,
5. history of multiple sexual partners (defined as more than 10 lifetime partners),
6. history of hemodialysis,
7. tattoo or repeated body piercing,
8. history of intranasal cocaine use,
9. unexplained liver disease,
10. unexplained/abnormal ALT,
11. intemperate or immoderate use of alcohol (defined as more than 50 g of alcohol per day for ten or more years.
-
“Screening Veterans for HCV Infection” and “HCV Risk Factor Assessment (Sample).”
n
2001
107
Congress
Veteran's
own
willful
misconduct
-
It
must
be
taken
into
consideration
that
the
Hepatitis
C
virus
penetrates
the
blood-brain
barrier
causing
an
array
of
mental
problems
that
impacts
veterans
lives.
Greater
than
60%
of
HCV
patients
suffer
from
conditions
such
as
"brain
fog,"
depression,
to
more
sever
disorders
that
include
bipolar
and
schizophrenic
behaviors.
Higher
numbers
suffer
from
chronic
fatigue
and
joint
pain
long
before
the
diagnoses
of
Hepatitis
C is
obtained.
Self
medication
though
alcohol
and
other
substances
is
common
place.
This
form
of
self-help
is a
death
warrant
for
the
vet.
Senate
version:
-
S 457 IS SNOWE
PRESUMPTION OF SERVICE-CONNECTION FOR CERTAIN VETERANS WITH HEPATITIS C ...establish a presumption of service-connection for certain veterans with Hepatitis C
(A) Period of service before December 31, 1992, a transfusion of blood or blood products.
(B) Exposed to blood on or through the skin or a mucous membrane during a period of service.
(C )Underwent hemodyalisis during a period of service.
(D) Experienced a needle-stick accident or medical event involving a needle, not due to the veteran's own willful misconduct, during a period of service.
(E) Diagnosed with unexplained liver disease during a period of service.
(F) Experienced an unexplained liver dysfunction value or test during a period of service.
(G) Served in a health-care position or specialty during a period of service under such circumstances as the Secretary shall prescribe for purposes of this subsection.
Referred to the Committee on Veterans' Affairs S.2599.IS > S 457 IS > S 1846 IS
Congress
version:
-
nH. R. 639 FRELINGHUYSEN
Veterans Comprehensive Hepatitis C Health Care Act 2001...testing and treatment of veterans for the Hepatitis C virus.¡(2) shall provide appropriate treatment for that veteran in accordance with the national protocol for the treatment of Hepatitis C .
n (A) each veteran who served in the active military, naval, or air service during the Vietnam era or who is considered to be `at risk,' and is enrolled to receive care under section 1710 of this title who requests the test or is otherwise receiving a physical examination or any care or treatment from the Secretary; and
n(B) to any other veteran who requests the test.
Referred to the Committee on Veterans' Affairs- H. R. 5132 >H. R. 639 > H. R. 73
-
The VA Hepatitis C Clinical Case Registry was created through the Center for Quality Management.
-
VA issued a solicitation for applications to establish Hepatitis C Resource Centers (HCRC). Four sites were funded: San Francisco, Northwest (Seattle, WA and Portland, OR), West Haven, CT, and Minneapolis, MN
-
Veterans’ National Hepatitis C Community Advisory Board was created with its first meeting in Washington DC
-
Briggs ME, Prevalence and risk factor for hepatitis C virus infection in an urban Veterans Administration medical center. Hepatology 34:1200-1205, 2001
The demographics of hepatitis C in United States civilians and VA patients are important. Several epidemiological studies have found hepatitis C to be higher in U.S. males, African-Americans, lower socioeconomic groups and in those Americans in the 40 to 60 year old age groups
-
We concluded that HCV is common in veterans. Risk factors independently associated with infection are IDU, prior transfusion, prior tattoo, combat medical work, incarceration, and multiple opposite sex partners. Infection with HCV among veterans is strongly associated with traditional risk factors for infection and less strongly associated with combat-related risk.
PMID: 11732010 [PubMed - indexed for MEDLINE]
In
2001
the
VA’s
goal
is
to
screen
all
veterans
who
have
not
been
screened
during
routine
clinic
visits
to
VA
medical
centers,
and
provide
treatment
when
it
is
appropriate.
In
fiscal
year
2001,
VA
received
$340
million
to
accomplish
this
goal,
however
VA
does
not
believe
it
will
spend
the
full
$340
million,
but
instead
will
spend
closer
to
$151
million.
Since
VA
does
not
expect
to
spend
$189
million
of
its
FY
2001
budget
allocations
on
HCV
costs,
it
has
lowered
the
request
for
fiscal
year
2002
budget
to
$171
million
to
treat
veterans
who
have
HCV.
The
cost
of
testing
and
treating
patients
for
HCV
is
high.
The
Washington
Post
(1/27/99)
quoted
Dr.
Kenneth
Kizer,
then
the
VA’s
top
doctor,
as
saying
the
new
testing
and
treatment
program
will
be a
controversial
“big
ticket
item”
costing
$12,000
to
$15,000
per
year
per
patient,
or
$250
million
to
$300
million
in
FY
1999
alone,
and
as
much
as
$500
million
in
FY2000.
“There
is a
huge
cost
that
is
involved,”
Kizer
was
quoted
as
saying.
“We
acknowledge
it,
but
I
don’t
know
what
choice
we
have.”
- GAO testimony before the Subcommittee on VA, HUD, and Independent Agencies, Committee on Appropriations. “Veterans’ Health Care: Observations on VA’s Assessment of Hepatitis C Budgeting and Funding” GAO-01-661T
DISCUSSION OF HEARING ISSUES
1. Why has screening and testing for Hepatitis C been limited and inconsistent?
GAO found several reasons why screening has been limited and inconsistent. According to GAO, local managers have adopted restrictive Hepatitis C screening policies because they were not aware specific funding was available to screen and test patients. GAO found instances where HCV screenings for risk factors were limited to a few clinics, on certain days of the week. In other instances, GAO found patient access to screening and testing was viewed as solely a matter of the individual physician’s judgment, not a matter of VA policy. In some cases providers were concerned about the costs of laboratory tests. As a result, they screened in primary care clinics on a rotating basis, one clinic per day.
While visiting the Northport VA Medical Center (VAMC), in Long Island, NY, GAO found the director was concerned about pharmacy costs relating to HCV treatment and the increased patient load the facility might incur because of the closure of the Health Maintenance Organizations (HMO) in the area. The Northport VAMC had limited HCV screening in one clinic, and no screening in specialty care clinics prior to FY 2001, but has since expanded HCV screening.
GAO’s visit to the Syracuse, New York VAMC found similar concerns about expenses. Syracuse providers expressed concerns about the cost of lab tests for HCV. As a result of these concerns, Syracuse patients were screened for HCV in primary clinics on a rotating basis, one clinic per day.
A second reason for the low rate of screening and testing veterans for HCV is attributed to weaknesses in facilities’ risk assessment procedures. GAO is concerned the screening process may discourage veterans from being candid about risky behaviors. Veterans are asked a series of questions relating to their sexual practices and drug and alcohol history which some may find invasive and embarrassing. If a patient admits to a risk factor, the provider will order testing. However, if a patient is not forthcoming about risk factors, providers will not test the patient unless the patient requests to be tested. GAO also found instances of screening for risk factors being conducted near public areas where a veteran’s answers might be overheard. Too-quick, routine administration of the HCV questionnaire amidst other screening procedures may also result in veterans not understanding the risk factors.
A third factor why many veterans remain undiagnosed, according to GAO, is weakness in testing procedures. GAO found instances of blood tests never ordered, or never completed, for veterans with risk factors.
In order to improve screening performance, GAO is expected to recommend VA set performance targets to convince providers HCV screening and testing is a high priority, and that VA provide definitive implementation guidelines regarding who should be screened and how screenings should be conducted.
Hearing witnesses from the VA will be asked what incentives are in place to encourage providers to increase the number of patients screened for HCV risk factors. VA is anticipated to testify the installation of the clinical reminder software will encourage providers to screen patients for HCV risk factors. However, while VA mandated clinical reminder software be installed by July 30, 2000, GAO found many instances where facilities were slow to turn on the software.
|
|
2002
|
|
2003
-
Department of Veterans Affairs’ recommendations for treatment of patients with cirrhosis were published on the VA’s Hepatitis C Web site
-
Toolkit for creating HCV support groups was published on the VA’s Hepatitis C Web site (www.hepatitis.va.gov).
-
Finally published after almost 2 years- VA Study 488- Elevated Prevalence of Hepatitis C Infection in Users of United States Veterans Medical Centers-
No risks specifically associated with military service or military combat were identified. ..In summary, we (the VA) estimate that 5.4% of VA users are HCV-seropositive, exceeding ...the general population by more than 2-fold. Although Vietnam veterans had the highest prevalence (11%) in our sample, military-related exposures were not found to be significant risk factors. That this estimate differs considerably from some prior estimates used to determine health policy...
According
to
the
study,
spending
2
days
in
the
local
jail
was
a
bigger
risk
factor
than
combat.
How the VA Used Study 488 to Deny Millions of Retired Military and Veterans Help.
 The study 488 is used for the bases of a questionnaire that decides the need to test Retired Military and Veterans for Hepatitis C. The study results show 7% of Veterans attending VA clinics, reported having Hepatitis C and receiving a Jetgun injection during service. However, some clinics didn't get the right survey. The wrong survey data did not included the Jetgun option. The study 488 is used for the bases of a questionnaire that decides the need to test Retired Military and Veterans for Hepatitis C. The study results show 7% of Veterans attending VA clinics, reported having Hepatitis C and receiving a Jetgun injection during service. However, some clinics didn't get the right survey. The wrong survey data did not included the Jetgun option.
Both, the wrong and new surveys, did address the lifestyle risk involving multiple partners. Jason A. Dominitz, et al, reports 5.5% association to infection, if the patient had between 2 and 49 partners. Ironically, this risk is listed to determine the need to test Vets, but the Jetguns, with a higher occurrence rate (7%), are not.
Study 488 IS flawed and diminishes the real need to test all Retired Military and Veterans
http://hcvets.com/data/transmission_methods/study488.htm More
-
Lennox Jeffers, a professor at the School of Medicine 2003 Between 10 and 15 percent of U.S. veterans are infected with HCV, which is a much higher prevalence than in the private sector.
-
Statement Of Lawrence R. Deyton, Md, Msph- Chief Consultant, Public Health Strategic Health Care Group- Veterans Health Administration- Department Of Veterans Affairs
Before The Committee On Government Reform
U. S. House Of Representatives
December 14, 2004
The Hepatitis C Case Registry is another important tool for quality improvement and programmatic planning. The objectives of the Registry are to identify VA patients who have been tested or diagnosed as having hepatitis C,...Through the end of FY 2004, over 273,000 unique patients had been added to the Registry. Of these, 184,067 had at least one VA inpatient admission or outpatient encounter in FY 2003.
-
Study- A comparison of hepatitis C treatment and outcomes at academic, private and Veterans' Affairs treatment centers states veterans attending VAMC clinics (click on link) Results: Differences in treatment practice and use of diagnostic procedures were found. Genotype testing was under-utilized in non-academic sites (academic centres, 79.2%; private centres, 33.7%; Veterans' Affairs centres, 35.9%; P < 0.001). Liver biopsies were performed less often in private sites (academic centres, 95.8%; private centres, 80.0%; Veterans' Affairs centres, 92.2%; P < 0.01). End-of-treatment viral response (academic centres, 40.0%; private centres, 31.3%; Veterans' Affairs centres, 17.2%; P < 0.05) was lower than that found in published trial data. Multivariate analysis revealed genotype 1 as the single significant predictor of treatment failure (P < 0.01).
|
|
2004
n
- 108 Congress H. RES. 633 UDALL
Expressing the sense of the House of Representatives 2004
Expressing the sense of the House of Representatives that there is a critical need to increase awareness and education about hepatitis C .
Mr. UDALL of New Mexico submitted the following resolution; which was "Whereas the majority of veterans infected are Vietnam era veterans , and the prevalence of infection is highest in this group"
Referred to the Committee on Energy and Commerce
-
Statement Of Lawrence R. Deyton, Md, Msph- Chief Consultant, Public Health Strategic Health Care Group- Veterans Health Administration- Department Of Veterans Affairs
Before The Committee On Government Reform
U. S. House Of Representatives
December 14, 2004
...As a result of these efforts, since 1999, over 4 million veterans in VA care have been screened for risk factors and over 200,000 were diagnosed with hepatitis C infection. During each of the past three years, screening and testing performance has been evaluated using the External Peer Review Program (EPRP), a national yearly review of approximately 50,000 medical records by trained, professional reviewers. The EPRP results have demonstrated steady improvement in screening and testing. In fiscal year 2004, over 98 percent of patients had been screened for risk factors, and over 90 percent of those at risk had been tested for or diagnosed with hepatitis C.
- Study: Analysis of a hepatitis C screening for US Veterans Dept. of Preventive Medicine, HSC Level 3, Rm. 086, SUNY at Stony Brook, School of Medicine, Stony Brook, NY 11794-8036, USA. In the multivariate model developed... service during the Vietnam era, tattoo, and a history of abnormal liver function tests were independent predictors of HCV infection. Our data support considering a more targeted screening approach that includes five of the 11 risk factors.
- Sloan KL, et al. Hepatitis C tested prevalence and comorbidities among veterans in the US Northwest. J Clin Gastroenterol 2004;38:279-284. 37,398 veterans from the VA health care system in the Pacific Northwest were tested for anti-HCV antibodies, and 8,230 (21.7%) were positive.(9) 45.8% of the seropositive veterans were between the ages of 40 and 49 years.
- 55th Annual Meeting of the American Association for the Study of Liver Diseases- David Bernstein, MD- Hepatitis C -- Current State of the Art and Future Directions CME- - Prevalence and Natural History- Trends in Hepatitis C Prevalence in the United States - ...One of the major shortcomings of this study (NHANES III survey) is that it reports on the prevalence of the hepatitis C antibody, which may indicate previous exposure or active disease. This study does not report on disease prevalence, as prevalence of hepatitis C infection is defined by the presence of hepatitis C viral RNA in serum. Only 148 of the 15,079 participants had serum available for hepatitis C viral RNA testing, making any statements regarding disease prevalence, and not potential exposure to the disease, invalid.
-
Hepatitis C: Silent Alarm Patent agreement draws federal review
©2004 The Kansas City Star
Chrion, like a dog with a bone when it comes to HCV, gets attention from Mike McGraw. Mike shows the federal lapse that allow a company to control a disease.
View Full Message
|
2005
nLast attempt by congress for a veteran's Presumed Service Connection bill
- 109 Congress H. R. 3434 ANDREWS
PRESUMPTION OF SERVICE-CONNECTION FOR CERTAIN VETERANS WITH HEPATITIS C ...establish a presumption of service-connection for certain veterans with Hepatitis C
(A) during a period of service before December 31, 1992, a transfusion of blood or blood products.
(B) exposed to blood on or through the skin or a mucous membrane during a period of service.
(C ) underwent hemodyalisis during a period of service.
(D) experienced a needle-stick accident or medical event involving a needle, not due to the veteran's own willful misconduct, during a period of service.
(E) diagnosed with unexplained liver disease during a period of service.
(F) experienced an unexplained liver dysfunction value or test during a period of service.
(G) served in a health-care position or specialty during a period of service under such circumstances as the Secretary shall prescribe for purposes of this subsection.
Referred to the Committee on Veterans' Affairs
HR 3455 IH > H. R. 3434
-
A CORRECTED ESTIMATE: FIVE MILLION AMERICANS INFECTED WITH THE HEPATITIS C VIRUS: A CORRECTED ESTIMATE- American Assoc for the Study of Liver Disease (AASLD) Nov 2005 Brian R. Edlin, Weill Medical College of Cornell University, New York, NY
-
General Hospital and Personal Use Devices Panel Meeting - August 9, 2005
Charles E. Edmiston, Jr., Ph.D., Chairperson, presiding.
During the panel meeting this question posed by Dr. Edmiston to MARTIN FRIEDE, Ph.D., Initiative for Vaccine Research, World Health Organization:
CHAIRMAN EDMISTON: If the devices are used in a compliant manner the way they're meant to be used, do you think the devices are safe?
DR. FRIEDE: The devices that we have seen without a protection cap, we have data from the calves and the data from the Hoffman study in Brazil to show that frequent contamination of the ejected did take place. And that contamination was clearly of a level of blood that we are convinced can carry disease. So the devices which do not have a protection cap which are to be used for giving intramuscular injection we are convinced that these carry a significant risk.
Meeting Highlights
Table of Contents
Yellow Fever vaccine via a jet injector
WHO- Jetguns Significant Risk
If bleeding nozzle should be resterilize
-
Hepatology. 2005 Jan;41(1):88-96. Links
Elevated prevalence of hepatitis C infection in users of United States veterans medical centers. Dominitz JA
Epidemiologic Research and Information Center VA Puget Sound Health Care System, Seattle, WA 98108-1597, USA. jason.dominitz@med.va.gov
Several studies suggest veterans have a higher prevalence of hepatitis C virus infection than nonveterans, possibly because of military exposures. The purpose of this study was to estimate the prevalence of anti-hepatitis C antibody and evaluate factors associated with infection among users of Department of Veterans Affairs medical centers... Military-related exposures were not found to be associated with infection in the adjusted analysis. In conclusion, the prevalence of hepatitis C in these subjects exceeds the estimate from the general US population by more than 2-fold, likely reflecting more exposure to traditional risk factors among these veterans.
- Dominitz, J., Boyko, E., Koepsell, T., Heagerty, P., Maynard, C., Sporleder, J. "VACooperative Study Group 488. Elevated Prevalence of Hepatitis C Infection in Users of United States Veterans Medical Centers," Hepatology. 41: 88-96: 2005
...Serving two days in jail, bigger risk factor than service
-
Study 488: Elevated Prevalence of Hepatitis C Infection in Users of United States Veterans Medical Centers
Dr. Jason Dominitz of the VA Puget Sound Health Care System completes a national hepatitis C prevalence study using "supposedly" rigorous scientific methodology to produce a statistically valid sampling of veterans receiving health care from VA. The purpose of the study was to estimate the incident, which is different than prevalence, of anti-hepatitis C antibody and evaluate factors associated with infection among users of VA medical centers. Veterans' infection rates were slashed and no association to service was found. Medical journals would not publish the study for almost 2 years because the VA would not submit the data to verify the legitimacy of the study. See 2003- Study 488
|
2006
- VA recommendations for treatment of patients with hepatitis C were published in the Journal of the American Gastroenterology Association
http://vaww.hepatitis.va.gov/vahep?page=prtop04-gd-2006-00
- A Veterans’ Hepatitis C Quality Management and Database Program that works with existing VA data systems, collecting and analyzing quantitative data on hepatitis C, utilization, and quality parameters in order to continually improve hepatitis C care and prevention. The Hepatitis C registry was launched in 2002 and provides facilities the ability to produce local reports and do their own quality control; the registry was revamped in 2006 to improve its utility for HCV clinicians. NOTE: Reports are available at: http://www.hepatitis.va.gov/vahep?page=prin-cmg-01
- POLICY: It is VHA policy that each VA Medical Center Director must designate a Hepatitis C Lead Clinician to be the principal point-of-contact for all clinical hepatitis C program information and reporting between the facility, the Clinical Public Health Program office, and other facility program offices
|
n
2007
Since the beginning of the National Hepatitis C Program, data have been collected through the External Peer Review Program (EPRP), a national chart review to track and monitor efforts. Results show that over 95 percent of people who come into VA for care have been screened for risk factors and over 90 percent of those persons found to be at risk have been tested for hepatitis C.
What Are
VA Risk Factors for Hepatitis C
Red Cross Risk Factors
Risk factors for VA service connection: Hepatitis Questionnaire
The source of infection is unknown in about 10 percent of acute (less than 6 months) hepatitis C cases and in 30 percent of chronic hepatitis C cases.
According to the VA website, as of 2007- 225,000 veterans who have been identified as having hepatitis C infection in VHA. Funding of the four HCRC programs has been renewed for an additional 5 years (through Sept 30, 2011).
- Am J Gastroenterol. 2007 Sep 25; [Epub ahead of print] Links
Outcome of Screening for Hepatitis C Virus Infection Based on Risk Factors
The prevalence of a positive HCV antibody in veterans who identified a risk factor was 7.3% (95% CI 6.6-8.0%). Among those diagnosed through the screening program (N = 260), 47% had chronic hepatitis C. Among patients with chronic HCV, 18% had evidence of advanced liver disease ...Forty-four percent were not immediate candidates secondary to medical or psychiatric comorbidities or active substance abuse.
- Dig Dis Sci. 2008 Jun;53(6):1693-8. Links
Hepatitis B and C among veterans on a psychiatric ward.
Tabibian JH,...Department of Psychiatry, West Los Angeles Veteran's Affair's Hospital, David Geffen School of Medicine, University of California jhtabib@ucla.edu -...Several risk factors were associated with exposure. Inpatient psychiatric veterans seem to have increased rates of hepatitis B and C exposure.
- Hepatitis C virus (HCV) six times likely to develop non-Hodgkin's lymphoma (NHL) Risk of Non-Hodgkin Lymphoma and Lymphoproliferative Precursor Diseases in US Veterans With Hepatitis C Virus- Hepatitis C virus infection confers a 20% to 30% increased risk of non-Hodgkin lymphoma overall, and a 3-fold higher risk of Waldenström macroglobulinemia, a low-grade lymphoma.
The Federal Response110 Congress
These little pieces mean something when your writing legislation.
H. R. 2552 TOWNS - WILSON
Hepatitis C Epidemic Control and Prevention Act
Referred to the Committee on Energy and Commerce
HR 3539 > HR 1290 > H. R. 2552 >
S 1445 IS KENNEDY-HUTCHISON
Hepatitis C Epidemic Control and Prevention Act 2007
Referred to the Committee on Health, Education, Labor, and Pensions
S. 1143 > S 521 IS > S 1445 IS
Congress makes the following findings:
(8) Conservative estimates place the costs of direct medical expenses for Hepatitis C at more than $1,000,000,000 in the United States annually, and such costs will undoubtedly increase in the absence of expanded prevention and treatment efforts.
This
section
does
not
mention
what
type
of
expanded
prevention
and
treatment
effort,
i.e.,
national
level,
high
risk
population
or a
well
defined
general
population,
etc.
Veterans
that
do
not
attend
VA
health
care
centers
will
not
be
notified
of
the
risk
for
the
Hepatitis
C
virus
infection.
This
act
is
no
"federal
response"
to
the
hepatitis
C
epidemic:(
1 in 5 Vietnam era retired military and veterans have hepatitis C
2008

Patients
were
put
at
risk,
health
officials
say,
when
a
syringe
would
be
reused
on
an
infected
patient
and
then
used
to
draw
anesthesia
from
vials
intended
for
just
one
patient.
The
vials
would
then
be
used
on
other
patients,
potentially
spreading
disease."
Oct.
06,
2008
Copyright
©
Las
Vegas
Review-Journal
PUBLIC
HEALTH
CRISIS:
Queries
irk
hepatitis
patients
Attorneys
telling
clients
not
to
reveal
past
drug,
sexual
activity
By
ANNETTE
WELLS
REVIEW-JOURNAL
It
was
never
the
Southern
Nevada
Health
District's
intent
to
embarrass
anyone
when
it
determined
what
questions
to
ask
former
patients
of
two
Las
Vegas
gastroenterology
clinics
regarding
their
past
risk
factors
for
hepatitis
B, C
and
HIV.
But
that's
what
attorneys
for
patients
who
tested
positive
for
hepatitis
C
are
saying
could
happen,
and
many
are
advising
their
clients
to
refuse
to
cooperate.
Read
More
http://www.lvrj.com/news/30506469.html
_____________________________________________________________________________
Military
Veterans
should
heed
this
advice
when
screening
for
hepatitis
c
compensations
from
the
Veterans
Administration.
Be
sure
to
point
out
reused
vials
were
used
along
with
the
jetguns
and
all
inoculations
received
in
service.
_____________________________________________________________________________
And
this
is
the
Newer
Improved
Version
of
the
Ped-O-Jet
Jetgun
used
by
the
military
with
reusable
vials-
Vaccine.
2008
Mar
4;26(10):1344-52.
Epub
2008
Jan
18.
Preventing
contamination
between
injections
with
multiple-use
nozzle
needle-free
injectors:
a
safety
trial.-
The
study
ended
early
because
the
protector
cap
needle-free
injector
(PCNFI)
failed
to
prevent
contamination
in
the
first
batch
tested
(8.2%
failure
rate).
How
can
you
Help?
File
a
claim!
|
|
|