By PAUL HARASIM / RJ
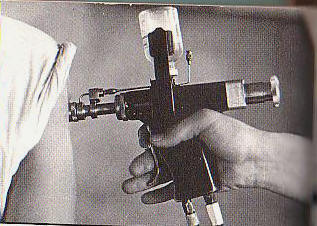
A number of veterans as
well as doctors now
believe that Vietnam
veterans...could have
contracted hepatitis C
through unsafe jet gun
vaccinations.
While it’s possible the government’s position on transmission of hepatitis C among boomers may have resulted in less testing, it’s critical today boomers forget any fears of stigma and get the easy blood test.